



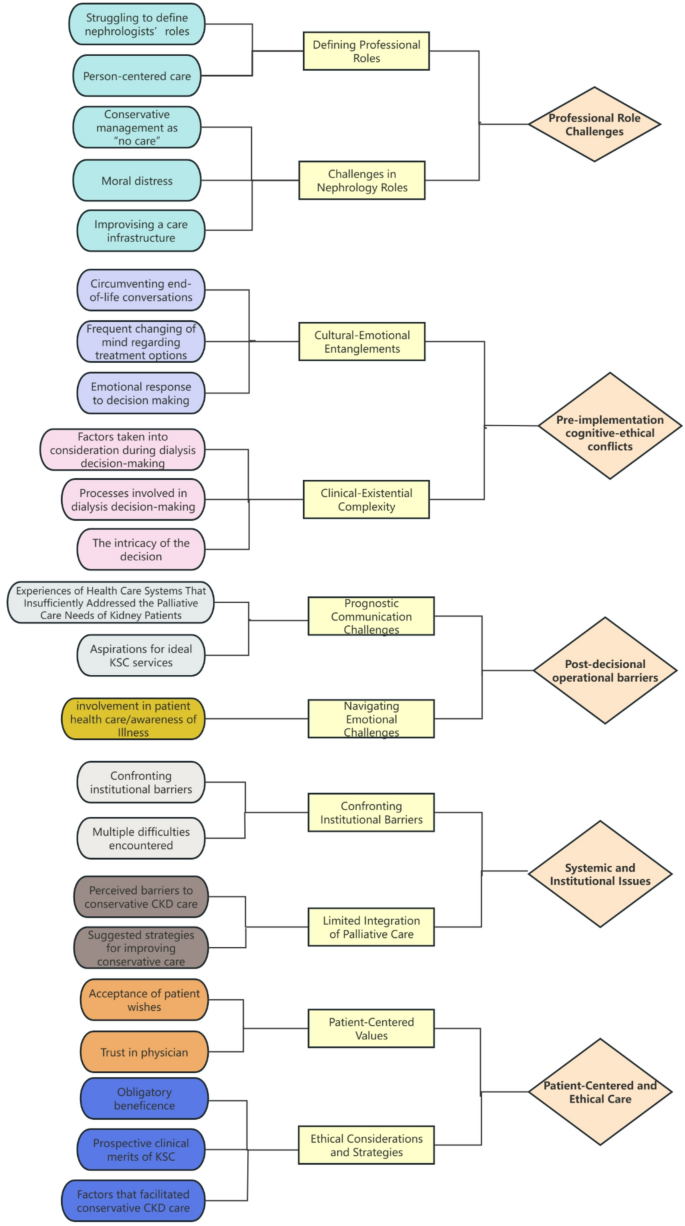
The final studies (25–32) comprised data from five countries: USA (3), UK (2), China (1), Australia (1), and Canada (1). The study cohort comprised 149 nephrologists, 80 nurses, 48 physicians, 15 allied health professionals, and 1 palliative care specialist. Of the eight studies incorporated in this research, seven are purely qualitative studies utilizing semi-structured interviews as the primary methodology, while the remaining one is a secondary qualitative study employing the secondary analysis of existing qualitative data. All included studies were original research articles published post-2016. Quality appraisal outcomes are presented in Tables 2 and 3 summarizes key extracted data. This study employs the PRISMA framework to report evidence synthesis outcomes. This systematic review identified five core themes characterizing clinicians’ perspectives on KSC implementation. The analysis revealed five core themes: Professional Role Challenges, Decision-making Dilemmas, The Challenges of End-of-Life Care Delivery, Systemic and Institutional Issues, Patient-Centered and Ethical Care. Thematic analysis generated distinct sub-themes, systematically organized in Fig. 2.

Theme 1: professional role challenges
Challenges in nephrology roles
The implementation of KSC in clinical practice presents significant challenges to healthcare professionals’ roles and responsibilities. KSC establishes a coordinated care framework requiring proactive patient-provider communication, contrasting traditional renal care models relying on discrete clinical teams managing fragmented care. This paradigm transformation is essential for optimizing care delivery and ensuring patient comprehension of clinically viable treatment pathways. Nephrologists must navigate transformative adaptations to conventional care paradigms amidst evolving clinical demands. A nephrologist highlighted the patient’s right to choose in decision-making, stating, “There are times when patients are not willing to make a decision, and as a patient, they have a right… because that’s their life, and if they do not want to decide what they want to do with end-stage renal disease (ESRD) imminent, they can do that.“[25] This statement highlights a critical tension in KSC implementation: while promoting shared decision-making, the model must also respect varying patient engagement preferences,, from deferral to refusal. Moreover, professional responsibilities are transforming in both scope and nature.
Another nephrologist also mentioned that they serve in informal or formal consulting roles in renal and/or palliative care clinics. “As consultants, our responsibilities could vary from advising other clinicians to co-managing patients with their primary nephrologists on a variety of issues including complex medical decision-making, advance care planning, and symptom management.“[30] While necessary, this evolution towards blurred professional boundaries and co-management in KSC highlights a key challenge for nephrology roles.
Defining professional roles
KSC implementation necessitates multidisciplinary collaboration with defined role clarity, structured communication protocols, and coordinated responsibilities to ensure care quality optimization. Clinicians encounter interprofessional communication barriers with nephrologists, particularly in patient co-management, stemming from role ambiguity and ineffective communication strategies. Primary care physicians advocate workflow-integrated frameworks, as one participant noted: “It takes an effort from the family or the primary care physician to actually liaise with the renal clinic to establish who does what and how do we do things.”[27] This quote highlights the ad hoc, effort-intensive nature of current role negotiation—a core challenge stemming from the absence of standardized frameworks for defining responsibilities and communication between primary and renal care teams. Nephrologists transitioning to KSC advisory roles require professional role adaptation, particularly when lacking prior dialysis-alternative decision-making experience. A nephrologist elaborated,“As consultants, our responsibilities could vary from advising other clinicians to co-managing patients with their primary nephrologists on a variety of issues including complex medical decision-making, advance care planning, and symptom management.”[30] This description illustrates the inherent fluidity of the Professional role. While essential for KSC, this fluidity also fuels the core challenge of role ambiguity.As a strictly standardized role definition has not yet been established in clinical practice, the acceptability and operational definition of this fluid role is likely to be significantly influenced by the prevailing professional hierarchies, team-based care norms, and formal care coordination mechanisms within the specific healthcare systems of different countries.
Theme 2: Pre-implementation cognitive-ethical conflicts
Cultural-emotional entanglements
Nephrologists recognize key KSC implementation barriers rooted in sociocultural factors. Inadequate patient/family understanding of dialysis and KSC principles impairs decision-making across disease progression stages.As exemplified by a family member’s misconception, “I get patients with mobility problems and dementia problems and vascular problems and their relatives believe that dialysis will cure all of the above.”[26] Familial involvement adds complexity by culturally mediating decision-making and emotional conflicts. In individualistic Western settings (e.g., UK), clinicians may exercise authority to alleviate familial guilt, as one nephrologist noted that excluding familial emotional considerations compromises evidence-based decision-making in dialysis withdrawal scenarios.“It is not upto you and I’m sorry you’d be angry with me or upset but it’s not up to you.”[32] This highlights varied implementation challenges: individualistic cultures (e.g., UK or US) prioritize exercising clinical authority. Conversely, in family-centric collectivist cultures (e.g., across Asia), familial decision-making predominates, with physicians often adopting deferential approaches. Consequently, KSC implementation and decision-making are significantly shaped by these Cultural-Emotional Entanglements. Concurrently, primary care physicians (PCPs) report limited awareness of renal conservative care resources [27], further impeding KSC adoption. These disparities reveal how cultural norms fundamentally shape implementation processes.
Clinical-existential complexity
During pre-terminal illness, clinical decisions are required for all therapeutic options, yet multimorbidity and individual needs add complexity into this process.As a Clinical Nurse Specialist stated, “This is one of the most complex areas in medicine to make decisions on, and it’s becoming more complex because of the types of patients we’re now being asked to deal with.These are patients that are elderly and frail, with lots of comorbidities, sometimes very severe, like dementia, cancer, and these are the decisions which are becoming really, really difficult to make, and no consultant I know can make these decisions easily. If they do make them easily, they’re doing it wrong. These decisions are extremely difficult. They have to be individualised for each patient. They take hours of talking. Very rarely is this decision easy in the majority of elderly frail patients. [29] This explanation illustrates clinical complexity—where multimorbidity and frailty impacts decision-making in progressive disease—challenging KSC’s goal of standardize care pathways while maintaining patient-centered flexibility. Nephrologists from five units reported being involved in regular multidisciplinary best interests meetings, involving clinicians, social workers and often the general practitioner, while others did not.We don’t have a discussion forum where we…or a multidisciplinary meeting where we discuss patients with these RRT decisions. [26] At a macro level, KSC decision-making reveals that variations in interdisciplinary support across nations reflect systemic healthcare differences. Countries with strong primary care integration (e.g., the UK) are better positioned to institutionalize such multidisciplinary forums. Conversely, fragmented systems often assign coordination to individual institutions.
Theme 3: Post-decisional operational barriers
Prognostic communication challenges
Prognostic communication with patients and families becomes increasingly complex as end-stage disease approaches, closely tied to cultural beliefs about mortality. These deeply held beliefs often lead to avoidance of end-of-life discussions, posing significant challenges for clinicians in conducting sensitive care transition dialogues. As clinicians acknowledge,“We are really, as a profession…so terrible at prognosis… To some extent it’s false optimism and realistic optimism and unwillingness to face death…also the realization that we’re just so terrible at predicting the future”[25] Doctor 2 observed, “Clinically, when broaching topics of mortality with patients or their kin, there’s a conspicuous predilection to circumvent these discussions.” These avoidance behaviors lead to a fundamental misalignment between KSC’s proposed palliative care paradigm and current clinical practice. The implementation gap is notably evident in East Asian cultural contexts where mortality discussions remain culturally proscribed, in contrast to more individual-oriented Western societies where KSC’s patient-centered approach faces distinct yet equally complex challenges during terminal care transitions.Similarly, Nurse 6 noted, “Rooted in our deep-seated familial values, numerous families find the decision to cease treatments profoundly challenging.[31] Thus, developing culturally adapted KSC guidelines that take for account documented cross-cultural differences in terminal care decision-making paradigms will be critical for enhancing implementation effectiveness during end-of-life prognostic communication and treatment transitions.
Navigating emotional challenges
The implementation of end-of-life EOL care is frequently challenged by healthcare providers’ negative emotional experiences, which stem from the complex interplay between communication barriers, emotional responses, and erosion of clinician-patient trust.As a US nephrologist described, “It was really challenging because I could tell that this family member was distrustful. I could tell that he felt like everyone was ‘trying to pull the plug on his mother.’ I really didn’t think it was good to dialyze her. I felt like it was really hard to get around that or to avoid doing it.”[32] Physicians face considerable ethical conflict when familial skepticism clashes with medical recommendations, with is further intensified in cultural contexts emphasizing collective family consensus over individual patient autonomy in healthcare decisions. A Clinical Nurse Specialist reported, “So they focus more on the bad side and what will happen to them because they think that once they have kidney failure, they die. There is no hope. So it depends on the staff, how you give them the information that will give them inspiration. We have this patient, but they are doing well’, so you kind of in a way encourage them as well, don’t tell them all the side effects, and you tell them ‘You are fit person – it could be good to you – you don’t scare them’.[29] As patients approach the end of life, KSC advocates for hospice care. However, cultural resistance to end-of-life discussions hinders clinicians’ ability to manege care transition conversations. KSC implementation must respect diverse cultural perspectives on mortality globally while addressing emotional challenges through regionally tailored communication frameworks.
Theme 4: systemic and institutional issues
Confronting institutional barriers
Currently, many healthcare systems lack established institutional frameworks to facilitate the clinical implementation of KSC. These systemic barriers not only exacerbate the challenges faced by clinicians but also significantly hinder broader understanding and adoption of KSC treatment strategies among stakeholders.“We talk about quality of life to the patients, we try to gauge what is important for them, but I do believe we do a poor jobbecause of the limits of time”[25] KSC implementation necessitates interprofessional collaboration, trust-building, and optimized communication within integrated health systems – critical success factors emphasized by nephrologists, “conservative management does take some collaboration between us and primary doctors and other supports. We as a nephrology division can’t do conservative management on our own, without any of those additional services to help out.”[25]Systemic deficiencies in palliative care infrastructure impede KSC integration into clinical practice. Nurse 3 opined, “Given that hospitals primarily focus on disease amelioration and life preservation, KSC’s widespread adoption seems implausible. Contemporary Chinese medical institutions typically relegate palliative endeavors to specialized hospices or dedicated wards. Propagating this care approach in top-tier hospitals remains fraught with complexities.”[31] The identified systemic barriers underscore fundamental disparities in palliative care adoption among nephrology patients globally. Leading medical centers in China and comparable healthcare systems persist in prioritizing disease-modifying interventions over palliative approaches, resulting in significant care quality disparities for end-stage renal disease patients. As the renal-palliative care field gains momentum globally, strategic resource reallocation is essential to to address disparities in care delivery.
Limited integration of palliative care
Current KSC clinical support remains constrained, manifested through insufficient palliative care integration and clinician training deficits within healthcare systems. A nurse delineates resource constraints as follows, “We would love to refer to palliative care for symptom management, but, when it actually comes to the crunch, neither of us have the resources to make it work”[28]. The constrained integration of palliative approaches with renal disease management creates significant implementation challenges, ultimately hindering the development and widespread adoption of KSC.
Doctor 3 highlighted a crucial distinction, “The nuances of palliative care for Renal ailments differ markedly from oncological palliation. The evolution of palliative care for ESRD lags, with palpable deficits in awareness among both patients and their families, posing challenges for KSC’s broad-based implementation.”[31] Resource limitations reflect systemic underfunding of palliative care frameworks in kidney disease management, highlighting the necessity for paradigm-shifting education to reclassify dialysis as an elective rather than mandatory intervention – a particularly formidable barrier in cultural contexts where palliative care remains socially stigmatized.
Theme 5: Patient-centered and ethical care
Patient-centered values
Clinicians recognize KSC’s clinical value in nephrology, prioritizing patient-centered approaches and integrating palliative care principles. Unlike palliative care, KSC emphasizes ethical principle centrality, enhancing patient acceptability and care accessibility. A nurse mentioned, “KSC is my link for palliative care for my patients, regardless of all the best plans you can make, it’s a nice, hopefully smooth transition.“[28] Nephrologists emphasized mandating documentation of patient-initiated dialysis refusal in clinical records. Clinicians emphasized systematic documentation of advance care planning directives and life-sustaining treatment orders. Clinicians acknowledged potential noncompliance with documentation protocols and accessibility challenges during emergent clinical scenarios. To handle these kinds of situations, some nephrologists described coaching patients on how to voice their preferences and communicate with other clinicians who might not be familiar with their goals. They also worked to build consensus among other clinicians and family members around supporting patients’ treatment preferences in order to increase the likelihood that patients’ wishes would be respected[30]. KSC’s transitional role addresses a critical gap in nephrology care, whereas traditional palliative models may be viewed as a form of surrender. Its ethical framework as active patient-centered care improves acceptability among dialysis-dependent populations. Its structured approach equips clinicians with practical tools to operationalize patient autonomy while sustaining therapeutic relationships.
Ethical considerations and strategies
KSC prioritizes ethical principles including beneficence and patient autonomy while advocating optimized conservative management strategies for CKD. The nephrologists whom we interviewed spoke of how clarifying patients’ preferences alone did not guarantee that they would receive the kind of care that they desired. Therefore, explicit strategies were developed to help patients ensure that their wishes were upheld when interacting with the wider healthcare system. These included educating patients about the signs and symptoms that they might develop and helping them to formulate a plan of action in the event of a health crisis[30]. While renal replacement therapy extends survival in ESRD patients, treatment-related morbidity and potential dialysis intolerance persist, particularly in elderly populations. KSC emphasizes QOL optimization and ongoing assessment aligned with disease progression over survival prolongation, thereby upholding life dignity. Therefore, a nurse emphasized the profound essence of KSC, affirming its significance, “Mere extension of life, devoid of inherent quality, borders on the futile. It’s imperative we uphold patient autonomy and prioritize quality in the terminal stages.”[31] KSC emphasizes ethical principles, such as beneficence and patient autonomy, while promoting optimized conservative management strategies for CKD. However, as our study’s nephrologists highlighted, simple clarification of patient preferences does not ensure goal-concordant care. By reframing “active care” as symptom management instead of dialysis persistence, KSC aligns with value-based care models emerging in Europe and North America.
link